

STORY AT-A-GLANCE
- COVID-19 is clearly no longer an emergency. The real emergency now is the continued use of the COVID “vaccines,” because they’re creating injuries on a level that is truly alarming and unprecedented. VAERS data reveal the COVID jabs have caused more harm in 18 months than all other vaccines on the market, combined, over the past three decades
- Raw data from the Pfizer trial also show the shots were associated with an increased risk for death from the start, and both Pfizer and the FDA knew it
- Data also show highly “vaccinated” and boosted nations are now experiencing record case and death rates from COVID compared to countries with low injection rates
- We’re now finding the COVID shots have negative efficacy, meaning, if you have received the shot and are exposed to COVID, you are more likely to get sick, not less likely, compared to someone who is unvaccinated
- The Frontline COVID-19 Critical Care Alliance (FLCCC) has developed a protocol for those injured by the COVID jabs called I-RECOVER, which you can download from covid19criticalcare.com in several different languages
In the “Tea Time” episode above, Drs. Pierre Kory and Paul Marik review the Frontline COVID-19 Critical Care Alliance (FLCCC) protocol for those injured by the COVID jabs. They also discuss what’s in the shots, their lack of safety and efficacy, adverse events, and the controversial issue of “shedding.”
Kory and Marik are both part of the FLCCC, which was founded in 2020 to share early treatment protocols for COVID-19. Kory is an ICU specialist, triple board certified in internal medicine, critical care and pulmonary medicine. He now runs a private tele-health practice specializing in the treatment of COVID-19, so-called “long-COVID” and vaccine injuries.
Marik is one of the most-published ICU specialists in the world, and best known for his vitamin C protocol for sepsis. The FLCCC’s protocol for COVID is known as the MATH+ protocol, which has undergone multiple revisions over the course of the pandemic.
Now, as injuries from the COVID jab are stacking up, they’ve also added a post-vaccine treatment called I-RECOVER,1 which you can download from covid19criticalcare.com in several different languages.
A Pandemic of Serious Vaccine Injuries
“My heart is so broken, I cannot keep quiet anymore,” Marik said, choking back tears during a Children’s Health Defense hearing in Ohio where several vaccine injured patients also shared their tragic journeys. “This is a humanitarian crisis! These people are suffering. This is real disease.”
Patients injured by the COVID jab repeatedly report receiving no help when they go to the hospital. There’s seemingly no help anywhere. This must change. We have to face the fact that we now have an unrecognized epidemic of vaccine injury.
At present, there are no specialized vaccine injury clinics, but eventually, there probably will be. In the meantime, the FLCCC is sharing their I-RECOVER2 protocol with the world, with the hopes that doctors will begin to take those with COVID jab injuries seriously and treat them appropriately.
As noted by Kory, COVID-19 is no longer an emergency. The real emergency now is the continued use of the COVID “vaccines,” because they’re creating injuries on a level that is truly alarming and unprecedented.
He also cites life insurance data showing historic rises in excess mortality among young people, and those data are supported by vaccine injuries reported to the U.S. Vaccine Adverse Event Reporting System (VAERS) as well. According to Kory, estimates suggest some 500,000 Americans may have lost their lives to these shots.

Data also show highly “vaccinated” and boosted nations are now experiencing record case and death rates from COVID compared to countries with low injection rates.
What’s in the Shots?
The short answer to that question is, “we have no idea,” and that puts medical professionals in a very precarious position. Since they do not know they’re giving their patients, they can’t even make educated recommendations based on the patient’s medical history, allergies and so on.
While the manufacturers have revealed some of the ingredients — such as mRNA, PEG and nanolipid particles — investigations have discovered things in the shots that aren’t indicated by the manufacturer. One such ingredient is graphene oxide, which can be seen under an electron microscope, but isn’t on the list of ingredients. Other unknown contaminants have also been found.
What’s more, while we know the shots contain “mRNA,” we have no way of knowing exactly what that mRNA is designed to do, or might accidentally do. As noted by Marik, it’s been genetically altered, so it’s not a direct copy of the mRNA found in the SARS-CoV-2 virus, but aside from that, we cannot be sure about its makeup.
Marik also points out the Pfizer data shows there are distinct differences in side effects depending on the lot you get. So, all lots are not the same. This basically makes it impossible to make definitive assertions about the ingredients, as any given lot may or may not contain them. The amount of any given ingredient may also vary.
Is the COVID Shot Safe and Effective?
When media and health officials say the shots are safe and effective, what does that actually mean? As noted by Kory, “safe and effective” is NOT a statement about a scientific conclusion. They’re “neither safe nor effective,” he says.
The “safe and effective” claim is simply propaganda and meets the definition of false information, because the data “backing” the safe and effective narrative completely ignore the adverse event data.
Kory notes we have documents showing the Department of Health and Human Services paid $1 billion to media companies to advertise the jabs. We also have evidence that first-tier journals are rejecting analyses of injuries. So, they’re very selective about what they publish.
Direct-to-consumer prescription drug ads accounted for $6 billion in spending alone in 2016, which amounted to 4.6 million ads, including 663,000 television commercials, mostly for high-cost biologics and cancer immunotherapies.3 It may be close to $10 billion now as that statistic is 6 years old. We know it is at LEAST $7 billion as the government kicked in $1 billion for COVID propaganda.
Public health agencies have also been very selective about the data they publish in order to protect the narrative. Health agencies in Scotland and the U.S., for example, suddenly stopped publishing data when the trend turned against the COVID shots and ineffectiveness and harms were becoming apparent.
Still, VAERS’ data reveal these jabs have caused more harm in 18 months than all other vaccines on the market, combined, over the past three decades. Raw data from the Pfizer trial — which were analyzed by experts after Pfizer and the Food and Drug Administration were sued and forced to release them — also show they were unsafe and associated with an increased risk for death from the start, and both Pfizer and the FDA knew it.
According to Marik, Moderna and Pfizer also manipulated their efficacy data to make the shots appear far better than they actually were. Recalculations have found the initial efficacy was actually more like 12%, not 95% as claimed, Marik says.
Don’t just survive — THRIVE! Prepper All-Naturals has freeze-dried steaks for long-term storage. Don’t wait for food shortages to get worse. Stock up today. Use promo code “jdr” at checkout for 35% off!
Negative Efficacy Demonstrated
Not only did the shots fail to live up to their initial claims of effectiveness, but we’re now finding they even have negative efficacy. As explained by Kory, negative efficacy means that if you have received the shot and are exposed to COVID, you are more likely to get sick, not less likely, compared to someone who is unvaccinated.
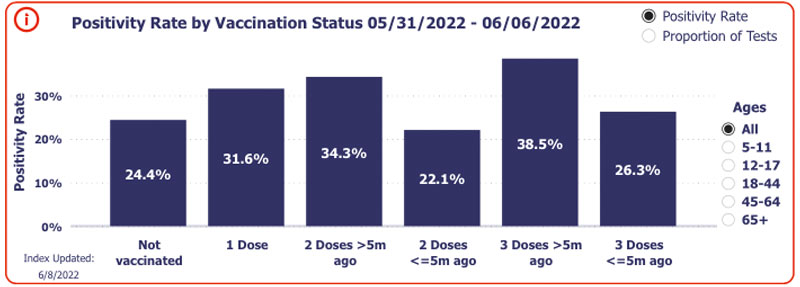
According to Kory, negative efficacy is demonstrated in several different data sources, including Walgreens, which created its own COVID tracker database for patients getting their tests and shots at Walgreens. Its data show COVID-jabbed individuals are testing positive for COVID at far higher rates than the unjabbed, and those who got their last shot five months or more ago have the highest risk.
As you can see in the screenshot from Walgreens’ COVID-19 tracker4 below, during the week of May 31 through June 6, 2022, 24.4% of unvaccinated individuals who got tested for COVID got a positive result. Of those who had gotten just one COVID shot, the positivity rate was 31.6%.
Of those who received two doses five months or more ago, 34.3% tested positive, and of those who received a third dose five months or more ago, the positive rate was 38.5%. “I’m very, very concerned for those who have been vaccinated and boosted,” Kory says.

Data from the U.K. Health Security Agency also show that the boosted now have three to four times higher COVID case rates, compared to the unvaccinated, and this is true for all age groups except children under 18.5,6 They’re also at greater risk of repeated COVID infections.
Do the COVID Shots ‘Shed’?
What about “vaccine shedding”? Marik admits to being extremely doubtful about the idea of spike protein shedding when he first heard about it, but has since changed his mind. He’s now convinced that it does happen, even though we do not yet fully understand the mechanism behind it.
He cites a study that looked at unvaccinated children of parents who had received the injections. The parents all had an antibody against the spike protein in their noses, and surprisingly, a large percentage of the unvaccinated children did as well. “So, somehow, the antibody is getting from the parent to the child,” he says.
Another concept that might explain it is that of exosomes. Exosomes are lipid particles that circulate in your blood. They’re also found in the nose and lungs. If you’ve received the COVID jab, you’re going to have circulating exosomes with spike protein on them, so it’s not inconceivable that you might spread these exosomes via nasal discharge or even just through breathing. “You could exhale these exosomes,” Marik says, “which are then inhaled [by others].”
Kory also points out that in the Pfizer trial, they included a “very curious exclusion criteria.” Anyone in the same household as someone who had received the shot was excluded from the trial, which suggests they may have been concerned about some sort of transfer or shedding.
Anecdotally, he has also encountered many unvaccinated patients, primarily women, who report severe disruptions to their menstrual cycles after coming into close contact (although not necessarily intimate contact) with someone who had recently received the jab.
Post-Jab Avalanche of Rare Diseases
Regardless of where the spike protein comes from — the virus itself, the shot or close contact shedding — it’s clear it can have wide-ranging adverse effects. The jab itself, however, is the most problematic, as your body is continuously producing this toxic protein, and we still don’t know if that production ever shuts off.
As previously predicted, we’re now starting to see a rapid rise in a number of conditions, including previously very rare ones. Among them, hepatitis among young children, appendicitis and several rare forms of cancer, some of which are extremely aggressive and fast-moving.
In late 2021, Dr. Ryan Cole, a pathologist, reported seeing a 20-fold increase in endometrial cancer, as well as a “massive uptick” in autoimmune diseases.7 (Not surprisingly, he’s now accused of misdiagnosing two patients with cancers they never had in order to support a false claim.8)
According to Kory, post-jab cancer proliferation is not all that surprising, as several of the mechanisms of the jabs degrade your immune function, and your immune system is your first line of defense against all disease, including cancer.
Marik also points out that the spike protein is “profoundly toxic” in and of itself as well, and interferes with cancer suppressing genes. “So, there’s no doubt that the spike protein causes an increase in the risk of cancer,” he says. “The problem is, what do you do about it? How do you get rid of the spike?”
Two Strategies to Eliminate Spike Protein
Marik and Kory believe there may be ways to boost the immune system to allow it to degrade and eventually remove the spike from your cells. One of the strategies they recommend for this is TRE (time restricted easting), which stimulates autophagy, a natural cleaning process that eliminates damaged, misfolded and toxic proteins.
In many ways Marik is a fairly rigid conventional physician who is simply unaware of many effective therapies natural physicians use. One major omission he is unaware of is sauna therapy. This is especially true when combined with TRE, as it will radically increase autophagy and heat shock proteins which will address the prion like diseases recently reported with COVID jabs and as predicted last year by MIT research scientist Stephanie Seneff.
Infrared saunas are clearly the best saunas out there as I detail in my epic article on sauna earlier this year. One of the primary reasons is the increase in mitochondrial melatonin.
Ivermectin also binds to the spike protein, thereby facilitating its removal. As noted by Marik, the best advice is to avoid the spike protein in the first place. Don’t take the COVID jab, and if you get COVID-19, treat it early and aggressively.
The spike protein is toxic regardless of whether it comes from the natural infection or the injection. Early and aggressive treatment will lower your spike protein load, thereby reducing your risk of long-COVID.
Kory stresses that, at present, they still do not know the exact correct dose for ivermectin. When prescribed for long-COVID and vaccine injury, he monitors the patient and adjusts the dosage based on individual response. That said, he typically starts patients out at a mid-range dose of 0.3 milligrams per kilogram of bodyweight, daily.
Now, he’s noticed that when it comes to ivermectin, there are responders and nonresponders. It works exceptionally well for some, while benefits are negligible in others. That said, a majority of patients do tend to experience a benefit. The length of treatment is also highly variable.
As for safety, it’s been used for over 50 years9 and has a remarkably robust safety profile. We now also have a large-scale Brazilian study in which patients received ivermectin for four days every month for six months. Curiously, not only was COVID incidence dramatically reduced, but kidney and liver function actually improved with this treatment. Marik also dismisses claims that ivermectin can be harmful to your liver, saying it’s actually used to treat fatty liver disease.
So, overall, “we have not seen a safety signal … with long-term use,” Kory says. “Some of that is published data, and some of it is just our experience with treating patients.” Marik adds, “It’s one of the safest medications … even when taken in high doses appropriately.”
FLCCC Vaccine Injury Protocol: First Line Therapies
The full first line protocol for vaccine injury is as follows. Keep in mind, however, that the treatment must be individualized to the symptoms of each patient. As explained by Marik, the patient’s response will determine future treatment and adjunct therapies. These are not symptom specific but rather listed in order of importance:10
Time Restricted Eating or periodic daily fasts. Fasting has a profound effect on promoting immune system homeostasis, partly by stimulating the removal of damaged cells and mitochondria and clearing misfolded and foreign proteins. Intermittent fasting likely has an important role in promoting the breakdown and elimination of the spike protein. Fasting is contraindicated in patients under 18 (impairs growth) and during pregnancy and breastfeeding. Patients with diabetes, as well as those with serious underlying medical conditions, should consult their primary care provider prior to fasting, as changes in their medications may be required and these patients require close monitoring.
Ivermectin — 0.2 to 0.3 mg/kg, daily for up to 4 to 6 weeks. Ivermectin has potent anti-inflammatory properties. It also binds to the spike protein, aiding in the elimination by the host. It is likely that ivermectin and intermittent fasting act synergistically to rid the body of the spike protein. Ivermectin is best taken with or just following a meal for greater absorption. A trial of ivermectin should be considered as first line therapy. It appears that patients can be grouped into two categories: i) ivermectin responders and ii) ivermectin nonresponders. This distinction is important, as the latter are more difficult to treat and require more aggressive therapy. Due to the possible drug interaction between quercetin and ivermectin, these drugs should not be taken simultaneously (i.e., should be staggered morning and night).
Low dose naltrexone (LDN) — Begin with 1 mg/day and increase to 4.5 mg/day, as required. May take 2 to 3 months to see full effect. LDN has been demonstrated to have anti-inflammatory, analgesic and neuromodulating properties.

Melatonin — 2 to 6 mg slow release/extended release prior to bedtime. Melatonin has anti-inflammatory and antioxidant properties and is a powerful regulator of mitochondrial function. The dose should be started at 750 mcg (μg) to 1 mg at night and increased as tolerated. Patients who are slow metabolizers may have very unpleasant and vivid dreams with higher doses.
Aspirin — 81 mg/day. (Please note: I do not agree with the routine use of aspirin, and recommend proteolytic enzymes such as lumbrokinase and serrapeptase on an empty stomach instead. Both serve to digest unwanted proteins in your blood, like blood clots. They also help combat inflammation and rebalance your immune system, facilitating the removal of inflammatory proteins, removing fibrin — a clotting material that restricts blood flow and prolongs inflammation — reducing edema in inflamed regions, and boosting the potency of macrophages and killer cells.)
Vitamin C — 1000 mg orally three to four times a day. Vitamin C has important anti-inflammatory, antioxidant, and immune-enhancing properties, including increased synthesis of type I interferons. Avoid in patients with a history of kidney stones. Oral Vitamin C helps promote growth of protective bacterial populations in the microbiome. It is important to note that these high doses are a pharmaceutical application of vitamin C and NOT recommended for daily use. It is far better to use whole food vitamin C and not ascorbic acid for daily use. I actually will be speaking with Dr. Marik and Korey September 9 and 10 at a vitamin C conference11 in Clearwater, Florida. If you come to the event you will be able to meet me personally there.
Vitamin D and Vitamin K2 — A dose of 4,000 to 5,000 units/day of vitamin D, together with vitamin K2 100 mcg/day is a reasonable starting dose. The dose of Vitamin D should be adjusted according to the baseline vitamin D level.
Quercetin — 250 to 500 mg/day (or mixed flavonoids). Flavonoids have broad spectrum anti-inflammatory properties, inhibit mast cells, and have been demonstrated to reduce neuroinflammation. Due to a possible drug interaction between quercetin and ivermectin, these drugs should not be taken simultaneously (i.e., should be staggered morning and night). The use of quercetin has rarely been associated with hypothyroidism. The clinical impact of this association may be limited to those individuals with preexistent thyroid disease or those with subclinical thyroidism. Quercetin should be used with caution in patients with hypothyroidism and TSH levels should be monitored.
Nigella Sativa — 200 to 500 mg twice daily. It should be noted that thymoquinone (the active ingredient of Nigella sativa) decreases the absorption of cyclosporine and phenytoin. Patients taking these drugs should, therefore, avoid taking Nigella sativa. Furthermore, two cases of serotonin syndrome have been reported in patients taking Nigella sativa who underwent general anesthesia (probable interaction with opiates).
Probiotics/prebiotics — Patients with post-vaccine syndrome classically have a severe dysbiosis with loss of Bifidobacterium. Kefir is a highly recommended nutritional supplement high in probiotics.
Magnesium — 500 mg/day.
Omega-3 fatty acids — DHA/EPA 4 g/day. Omega-3 fatty acids play an important role in the resolution of inflammation by inducing resolvin production.
FLCCC Second Line Therapies for Vaccine Injury
Adjunctive and/or second line therapies in the FLCCC’s vaccine injury protocol are:
Hydroxychloroquine (HCQ) — 200 mg twice daily for 1–2 weeks, then reduce as tolerated to 200 mg/day. HCQ is the preferred second line agent. HCQ is a potent immunomodulating agent, and is considered the drug of choice for systemic lupus erythematosus (SLE), where it has been demonstrated to reduce mortality from this disease. Thus, in patients with positive autoantibodies or where autoimmunity is suspected to be a prominent underlying mechanism, HCQ should be considered earlier. Further, it should be noted that SLE and post-vaccine syndrome have many features in common. HCQ is safe in pregnancy; indeed, this drug has been used to treat preeclampsia. With long term usage, the dose should be reduced (100 or 150 mg/day) in patients weighing less than 61 kg (135 lbs).
Intravenous vitamin C — 25 g weekly, together with oral Vitamin C 1000 mg (1 gram) 2–3 times per day. High dose IV vitamin C is “caustic” to the veins and should be given slowly over 2–4 hours. Furthermore, to assess patient tolerability the initial dose should be between 7.5–15 g. Total daily doses of 8–12 g have been well-tolerated, however chronic high doses have been associated with the development of kidney stones, so the duration of therapy should be limited. Wean IV vitamin C as tolerated.
Non-invasive brain stimulation (NIBS) — NIBS using transcranial direct current stimulation or transcranial magnetic stimulation has been demonstrated to improve cognitive function in patients with long COVID as well as other neurological diseases. NIBS is painless, extremely safe, and easy to administer. It is a recognized therapy offered by many Physical Medicine and Rehabilitation Centers. Patients may also purchase an FDA-approved device for home use.
Fluvoxamine — Start on a low dose of 12.5 mg/day and increase slowly as tolerated.
“Mitochondrial energy optimizer” with pyrroloquinoline quinone (e.g., Life Extension Energy Optimizer or ATP 360®).
N-acetyl cysteine (NAC) — 600–1500 mg/day.
Low dose corticosteroid — 10–15 mg/day prednisone for three weeks. Taper to 10 mg/day and then 5 mg/day, as tolerated.
Behavioral modification, mindfulness therapy, and psychological support — May help improve patient’s overall well-being and mental health. Suicide is a real problem in the vaccine-injured patient. Support groups and consultation with mental health professionals are important.
Tai Chi and Yoga — Tai Chi, a health-promoting form of traditional Chinese martial art, has shown to be beneficial for preventing and treating diseases including long COVID. Yoga has immunomodulating properties that may be beneficial in vaccine-injured patients. It should be noted that long COVID is characterized by severe post-exertional fatigue and/or worsening of symptoms, therefore patients should be counseled to moderate exertion, increasing slowly only as tolerated.
Examples of third line therapies and other potential remedies include hyperbaric oxygen therapy, whole body vibration therapy, cold hydrotherapy, nutraceuticals such as dandelion and broccoli sprout powder and carbon 60 (C60 fullerenes). For the full list, see the I-RECOVER Post-Vaccine Treatment Protocol12 available on covid19criticalcare.com.13
- 1, 10, 12 FLCCC I-RECOVER Post-Vaccine Treatment Protocol (PDF)
- 2 FLCCC I-Recover: Post Vaccine Treatment
- 3 JAMA. 2019;321(1):80-96. doi:10.1001/jama.2018.19320
- 4 Walgreens COVID-19 Index
- 5 The Defender May 4, 2022
- 6 UK Health Security Agency COVID-19 Vaccine Surveillance Report Week 13
- 7 Life Site News September 13, 2021
- 8 Idaho Capital Sun May 6, 2022
- 9 Proceedings of the Japan Academy Series B February 10, 2011; 87(2): 13-28
- 11 VCICI 2022 Conference
- 13 Covid19criticalcare.com
